
Estimated reading time: 11 minutesHeadaches and migraines are among the most common and disabling symptoms people with hEDS and HSD face.
Research suggests that migraines impact anywhere from 40-75% of people with hypermobility conditions, which is far higher than the general population that experiences migraine at a rate of 14% globally (1).
They also tend to be more severe, more frequent, and harder to treat than those without hypermobility (2, 1).
I’ve suffered headaches & migraines for as long as I can remember. I must have had headaches at a young age because I have a vague memory of asking for orange-flavoured aspirin from my mum.
The real issues started when the migraines began when I was 19 and just started work in an office. They happened every day and came with an aura, nausea, and sickness. They always arrived with my menstrual cycle, tiredness, or stress.
I’ve learnt to manage them with movement, meditation, cranial sacral therapy, and medication. Being post menopausal now, I think they are slowing down, but I have sympathy with anyone who lives with this condition.
As Dr. Katy Munro, Senior GP Headache Specialist at the National Migraine Centre, put it during a Zebra Club member event:
“There’s no such thing as a normal headache. The symptom of headache needs a diagnosis — you would never say ‘I just get the normal fever’ or ‘I just get the normal rash,’ because everybody knows those are symptoms of something else.”
Key Takeaways
- Headaches and migraines are among the most common and disabling symptoms in hEDS and HSD, and are often one of the first signs that something is wrong.
- Migraines in hypermobility tend to start earlier, occur more often, and be more severe than in the general population.
- There are many possible causes, including migraine, upper cervical instability, dysautonomia, TMJD, and cervicogenic headache — and they often overlap.
- Coat hanger pain is a well-recognised pattern in this community and is thought to be connected to dysautonomia and posture.
- Movement, breathing, nervous system regulation, and posture awareness can all support headache management alongside medical care.
- If your headaches are new, severe, or accompanied by neurological symptoms, please work with your medical team.
Updated June 2026
Are headaches common in hEDS and HSD?
Headaches are one of the most common and disabling symptoms in hEDS and HSD. They are also one of the first symptoms diagnosed, or signs that something is wrong (3, 1).
In a study of people with hypermobility disorders, 66% had head and neck problems, including headaches, neck pain, facial pain, neck instability, or a combination of these (4). For almost a third of them this was the primary reason for seeking help.
One pattern that comes up often in this community is coat hanger pain. It is a deep aching across the shoulders, upper back, and base of the skull that frequently accompanies or precedes a headache. It is thought to be connected to dysautonomia and posture, and it is recognisable enough that many people name it before they have a clinical explanation for it.
So it’s clear that if you are experiencing headaches, not only are you not alone, but you are with the majority of hypermobile individuals.
Why do people with hEDS and HSD get headaches?
There is no one reason why people with hypermobility get headaches. There are multiple causes that frequently overlap. The connection between connective tissue and various headache types is not always understood (3, 1, 4, 5).
Migraine is a common headache type in our population, and this will be covered in the next section. Beyond migraine, upper cervical instability (including craniocervical instability or CCI) is a significant contributor. This is due to ligament laxity impacting the joints at the top of the spine that can trigger or worsen headaches (6).
Dysautonomia, particularly Postural Orthostatic Tachycardia Syndrome (POTS) and orthostatic hypotension (OH), is another major contributor to headaches. When the autonomic nervous system struggles with regulating the blood flow to the brain when standing it makes sense that headaches would occur (1).
Temporomandibular joint disorders (TMJD) are also common in hypermobility and can cause significant head and facial pain (3, 5).
Other causes include tension type headache, cervicogenic headaches arising from the neck like occipital neuralgia, Chiari malformation and idiopathic intracranial hypertension (increased pressure of cerebrospinal fluid (3, 1, 5).
Medication overuse headache is also worth noting because many of us are at a higher risk because of the frequency of headaches and the presence of other pain contributors.
Anecdotally, we could probably add sleep issues, menopause, and mast cell activation syndrome (MCAS) as common issues that likely contribute to headaches.
It is important to say that not everyone with hEDS or HSD will experience all of these, and this list is not a diagnostic tool. If you are concerned about your headaches, particularly if they are new, severe, or accompanied by neurological symptoms, please work with your medical team to identify what is driving them for you specifically.

What makes migraines in hypermobility different?
Migraines in hypermobility can be more severe, more frequent, and apparently harder to treat than those in the general population. They are also often undertreated because the connection with hypermobility is underrecognized (2, 1).
A migraine is more than a headache. This condition is characterized by frequent moderate to severe attacks that last 4-72 hours. They are often one-sided, pulsating, and can be associated with nausea, light and noise sensitivity, and can be disabling (5). These may sound familiar because they often overlap with broader hEDS/HSD symptoms. Migraines, like hypermobility, are more common in women (5).
Migraines are considered chronic if there are attacks for 15 or more days a month, for more than 3 months, with “migrainous features” for 8 days a month or more (1). In hypermobile people specifically, migraines tend to start earlier in life, happen more often, have more severe symptoms, and are more likely to become chronic over time (2).
Several things help explain why. Dysautonomia is a significant factor: migraine, POTS, and hypermobility overlap more than is often recognised, and all three are frequently present in the same person (7).
Central sensitisation is another contributor because the nervous system in hypermobile people can become sensitised and, as a result, be more sensitive to pain stimuli and experience an amplified response to pain signals, making attacks more likely and more intense (8). Cervical instability also plays a role, as laxity in the neck joints can activate pain pathways that feed into migraine (8, 6).
Managing migraine in hEDS and HSD usually means looking at the whole picture, not just the headache. Movement, sleep, nervous system regulation, and lifestyle factors all make a difference to how often attacks occur and how severe they are (1).
If your migraines have been difficult to manage, it is worth seeking out a neurologist with experience in both migraine and connective tissue disorders, because the approach may need to be different from standard migraine treatment. This is a conversation worth having with your headache specialist.
As Dr. Katy Munro, Senior GP Headache Specialist at the National Migraine Centre, said at a Zebra Club member event: “Even if a person with migraine follows all the lifestyle suggestions, they may still suffer attacks, and it still isn’t their fault.” And on severity: “Migraine attacks can be mild. It’s a spectrum.” Both are worth remembering in a community that often holds itself to an impossible standard.

What are vestibular migraines, and how do they relate to hypermobility?
Vestibular migraine is a type of migraine where dizziness or vertigo is the primary symptom, often without a significant headache (9). I have a handful of clients who experience this, and it does complicate the headache picture.
The vestibular system’s job is to detect where the head is in space and how it is moving. This is done through nerve signals between the vestibular system in the inner ear and the brain. When migraine affects this system, the result can be vertigo, balance problems, and dizziness rather than, or alongside, head pain.
Vestibular migraine affects around 1% of the general population, with higher rates seen in specialist dizziness clinics (9). We currently have no specific prevalence figures for hEDS and HSD, though dizziness and balance difficulties are commonly reported in this community, particularly in people who also have dysautonomia (1).
To meet the diagnostic criteria, a person needs to have episodes of moderate to severe vestibular symptoms lasting 5 minutes to 72 hours, with at least one migrainous feature during at least half of the vestibular episodes.
These features include one-sided pulsating headache, light or sound sensitivity, or aura. Other causes of vestibular symptoms need to be ruled out (9).
Some examples of vestibular symptoms include internal vertigo (sensation that the body is in motion), external vertigo (sensation that the room is spinning), positional vertigo with changes in head position, visually induced vertigo, vertigo with head motion, and head motion-induced dizziness with nausea (9).
Vestibular migraines, like other migraines, are more common in women. They also seem to have an autosomal dominant inheritance pattern similar to that seen in hEDS, meaning a child of a parent has a 50% chance of inheriting the condition (10).
It was also interesting to learn that in postmenopausal people, typical migraines are sometimes replaced by episodes of vertigo, dizziness, or feeling off balance (10).
If you think you may be experiencing vestibular migraines, this is worth discussing with a neurologist or a specialist in vestibular migraine, sometimes a neuro-otologist or ENT. Vestibular rehabilitation with a physiotherapist experienced in this area may also help.
What is upper cervical instability and how does it cause headaches in hEDS and HSD?
Upper cervical instability (UCI) is a condition where the joints at the top of the spine, where the skull meets the neck, are excessively mobile due to ligament laxity. You may also hear it called craniocervical instability or CCI.
In this community it often shows up as neck instability headaches, base of skull headaches, or that familiar ache at the back of the head.
In 2023, the scientific advisor to The Zebra Club, Dr. Leslie Russek, published the first expert consensus and recommendations for screening for and managing Upper Cervical Instability (UCI) along with an international team of physical /physiotherapy clinicians and researchers, and a hypermobility specialist rheumatologist (6).
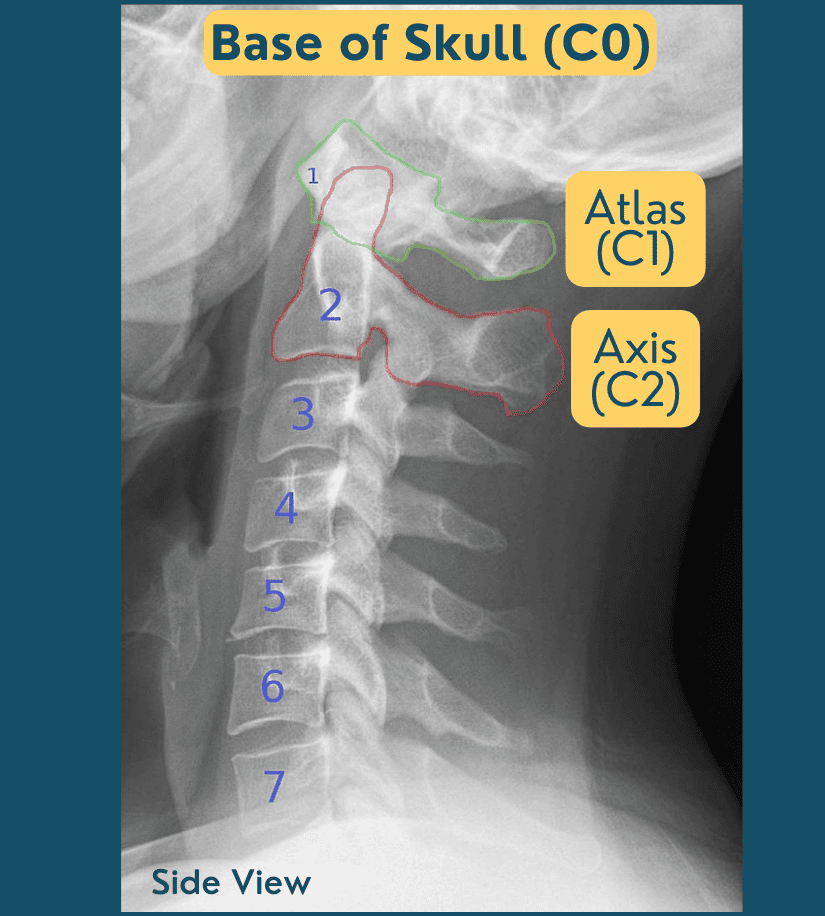
It helps to understand the anatomy. Craniocervical instability refers to ligament laxity in the joint between the base of the skull (C0) and the atlas (C1). There can also be instability between the atlas (C1) and the axis (C2), called atlantoaxial instability (AAI). Together these fall under the umbrella of upper cervical instability.
Mild UCI is relatively common among people with hEDS/HSD, impacting between 52-66% of people. Severe UCI is much less common, impacting only 5% of people with hEDS/HSD (6).
Symptoms of UCI exist on a spectrum and can include headaches, neck or facial pain, dizziness, vertigo, nausea, numbness/tingling, shortness of breath, difficulty speaking, vision changes (blurred, tunnel vision, auras), hearing changes, difficulty swallowing, choking, sleep apnea, memory deficits, pre-syncopal episodes (feeling like you’re going to faint) (6).
How is upper cervical instability identified?
I do not recommend trying to work this out yourself. Assessing for UCI requires a physiotherapist or clinician with experience in hypermobility, using specific clinical tools.
Dr. Russek and colleagues provide detailed guidance for clinicians on how to screen, assess, and manage UCI in people with symptomatic hypermobility (6). If you are concerned, finding a physiotherapist experienced in hEDS and HSD is the right first step.
According to the Russek et al. consensus guidelines, a clinician would be looking for three things: symptoms consistent with musculoskeletal or neurological UCI; symptoms that change with neck movement or position, for example worsening when looking down, flexing, extending, or rotating the neck; and findings on physical examination that suggest mechanical irritability (6).
Importantly, irritability can vary from day to day, and a good clinician will factor that in rather than making a judgment based on a single assessment.
More recent work applying these guidelines in practice found that an approach focused on body awareness, proprioception, and movement re-education supported meaningful improvement in people with highly irritable UCI (11)
What can help with headaches and neck pain in hypermobility?
There are many strategies that can genuinely help with headaches and neck pains, and many of these approaches I have used with my clients and have built into The Zebra Club Platform.
For UCI specifically, Russek et al. outline a range of interventions organised by levels of irritability (6). Much of what they recommend aligns closely with what I have found useful in practice.
Relaxation and autonomic nervous system regulation, particularly approaches that do not require neck movement, are a good place to start. Breathing is one of the most accessible tools here.
Slow whole body breathing can shift the nervous system out of a threat response, and there are breathing classes in The Zebra Club platform, as well as a free one you can try here. The Head, Neck, and Shoulders Meditation audio in The Zebra Club is something members regularly tell me helps with headache and coat hanger pain.
From there, building body awareness in different positions helps you notice what your body is telling you before symptoms escalate.
Posture also matters more than most people expect. How you sit, stand, and sleep affects neck load and headache frequency in ways that are worth paying attention to. This can also not be forced, or it may increase pain. I find it comes from a whole body approach working on all of the integral movement method principles.
Pain neuroscience education and mindful use of language to support feelings of safety are also part of the picture, alongside a personal self-care toolkit that might include TENS, topical pain relief, and relaxation strategies.
When it comes to migraine attacks, timing matters. As Dr. Katy Munro, Senior GP Headache Specialist at the National Migraine Centre, said at a Zebra Club member event: “If you do get a migraine attack, get on it quickly. The trouble with waiting to see if it’s a bad one is that it’s more likely to be a bad one if you leave it, because the migraine attack will roll and gather momentum, and then you will have missed the boat.”
This is worth discussing with your neurologist or GP so you have a personal plan in place.
Members of The Zebra Club can learn more about upper cervical instability and migraine in the Expert Insights section, where we have presentations by Dr. Leslie Russek (2023) and Dr. Ann McCarthy (2025), both authors on the UCI guidelines paper, and Dr. Katy Munro, Senior GP Headache Specialist at the National Migraine Centre, who joined us in July 2025.
Video: The Hypermobile Neck – CCI, Pain & Stability Exercises
In this video, I discuss more about my experience working with clients who have neck pain and headaches. I then teach a movement class. Please note – these exercises may not be suitable for everyone.
They should not cause increased pain or neurological symptoms. Please seek medical advice if they do. They are not designed to replace any medical guidance you have been given. If you are highly irritable in the neck, please work one-on-one with a physical therapist.
FAQ
Does hypermobility give you headaches?
Yes. Headaches are one of the most common and disabling symptoms in hEDS and HSD. They can result from many causes including migraine, upper cervical instability, dysautonomia, TMJ disorder, and muscle tension.
How to get rid of EDS headaches?
There is no single fix because EDS headaches have multiple causes. Addressing posture, breathing, nervous system regulation, and movement can help alongside medical support. Working with an EDS-aware clinician to identify your specific causes is the most important step.
What does EDS do to the brain?
EDS can affect the nervous system through issues with blood flow, autonomic function, and structural factors. These can contribute to symptoms like brain fog, dizziness, and headaches. If you have concerns about neurological symptoms, please seek medical assessment.
Are headaches common in EDS?
Yes. Headaches are one of the most frequently reported symptoms in hEDS and HSD and can occur for many different reasons, including migraine, upper cervical instability, dysautonomia, TMJ disorder, and cervicogenic headache.
Why do people with hypermobility get headaches?
Headaches in hypermobility have several different causes, including migraine, upper cervical instability, dysautonomia, TMJD, and muscle tension. These often overlap, which is part of why they can be so difficult to manage.
What kind of headaches do people with EDS have?
People with hEDS and HSD can experience many types, including migraine, cervicogenic headaches arising from the neck, tension headaches, vestibular migraines with dizziness, and headaches related to dysautonomia or raised intracranial pressure.
Are migraines common with EDS?
Yes. Migraines are significantly more common in people with hEDS and HSD than in the general population. They also tend to start earlier, occur more frequently, and be more severe. They are often undertreated because the hypermobility connection goes unrecognised.
Can hEDS cause migraines?
Migraine is significantly more common in people with hEDS and HSD than in the general population, and the two conditions frequently co-occur. Whether hypermobility directly causes migraine is not fully understood, but dysautonomia, cervical instability, and central sensitisation are all thought to play a role.
What is coat hanger pain and is it related to EDS headaches?
Coat hanger pain is a pattern of aching across the shoulders, upper back, and neck that is common in people with dysautonomia and hypermobility. It can accompany or precede headaches, particularly those related to posture and autonomic function.
What is a cervicogenic headache in EDS?
A cervicogenic headache originates in the neck rather than the head. In people with hEDS and HSD, neck hypermobility and instability can trigger these headaches, which often radiate from the base of the skull forward. An EDS-aware physiotherapist can help.
Can POTS cause headaches?
Yes. POTS, which is common in hEDS and HSD, can cause headaches particularly when standing or changing position. These orthostatic headaches may improve when lying down and often improve with dysautonomia management.
Does occipital neuralgia occur with EDS?
Occipital neuralgia is a type of headache characterised by sharp or shooting pain at the back of the skull. It can occur in people with hEDS and HSD, possibly related to neck instability or muscular tension. Medical assessment is recommended to confirm the cause.

Jeannie Di Bon is a movement therapist, educator and author specializing in hypermobility, Ehlers-Danlos Syndrome and chronic pain. She is the founder of The Zebra Club app and the creator of the Integral Movement Method.

Catherine Nation, MS, PhD, holds a Master of Science in Biological Sciences and a doctorate in Tropical Medicine and Parasitology. As Marketing Content Manager at The Zebra Club and a member of the hEDS community, she applies her scientific background to making complex research accessible and accurate.
Works Cited
- Mehta et al. (2024). Headache disorders in patients with Ehlers-Danlos syndromes and hypermobility spectrum disorders. Front. Neurol. 2024;15:1460352.
- Puledda et al. (2015) A study of migraine characteristics in joint hypermobility syndrome a.k.a. Ehlers-Danlos syndrome, hypermobility type. Neurol Sci. 2015;36(8):1417-1424.
- Levy et al. (2020) An investigation of headaches in hypermobile Ehlers-Danlos syndrome. Annals of Psychiatry and Clinical Neuroscience. 2020;3(3):1034.
- Malhotra et al. (2020) Headaches in hypermobility syndromes: a pain in the neck? Am J Med Genet A. 2020;182(12):2902-2908.
- Henderson et al. (2017) Neurological and spinal manifestations of the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):195-211.
- Russek et al. (2023). Presentation and physical therapy management of upper cervical instability in patients with symptomatic generalized joint hypermobility: international expert consensus recommendations. Front Med (Lausanne). 2023;9:1072764.
- Collins et al. (2025) Autonomic symptom burden, comorbidities and quality of life in women with hypermobility spectrum disorders and hypermobile Ehlers-Danlos syndrome. Autonomic Neuroscience. 2025;262:103356.
- Natbony LR, Ray CN (2025) Hypermobility spectrum disorders and migraine: screening matters. Practical Neurology.
- Lempert et al. (2022) Vestibular migraine: diagnostic criteria. J Vestib Res. 2022;32(1):1-6.
- Stolte et al. (2015) Vestibular migraine. Cephalalgia. 2015;35(3):262-270. doi:10.1177/0333102414535113
- Chalela S, Russek LN. (2024) Presentation and physical therapy management using a neuroplasticity approach for patients with hypermobility-related upper cervical instability: a brief report. Front. Neurol. 2024;15:1459115.

10 Comments
Laura Parsons - 10th June 2026
There’s also this; compression syndromes are becoming more recognized;
https://doi.org/10.1159/000537705
Jeannie Di Bon - 10th June 2026
Thank you for sharing this. This relationship is often multifactorial and under recognised so good to mention it here.
Johanna - 13th December 2025
Thanks for this informative Video ! Do You have any Tipps in sleeping? As my Pain already accurs directly in the Morning.
Jeannie Di Bon - 16th December 2025
Yes we do – there is a blog on sleeping here too.
Sleeping with hypermobility: A comprehensive guide
Sandra Smith - 5th March 2025
Any help with headaches that only start when I’m sleeping and occur nightly
Jeannie Di Bon - 7th March 2025
It is always best to consult with a medical professionals about any new types of headaches. Hope you have someone you can see for a medical consult.
Martina Ingemarsson - 10th April 2024
This article was very helpful to me, thank you! Very pedagogical. I will now make sure to watch the YouTube episode and class.
Jeannie Di Bon - 11th April 2024
Thank you – I am so glad you enjoyed this headache article.
Kylie - 29th March 2024
My daughter often tells us she is seeing one colour could be pink, blue, red or green then after a little while states she has a headache. Just interested what category this may fall into
Jeannie Di Bon - 2nd April 2024
Thank you for taking the time to comment. I cannot give any medical advice on here but do recommend checking with your medical practitioner.